
EHJ:荟萃分析显示降低高血压死亡率ACEI优于ARBs
2012-04-27 MedSci MedSci原创

Laura C van Vark博士(荷兰伊拉斯姆斯大学医学中心)和他的同事在他们发表于2012年4月17日《欧洲心脏病杂志》[European heart journal.2012-04-17.]的一项新的荟萃分析表明,与同一时期的应用非ACEI类药物或血管紧张素受体阻滞剂等药物(ARBs)的患者相比应用ACEI类药物的高血压患者的全死因死亡
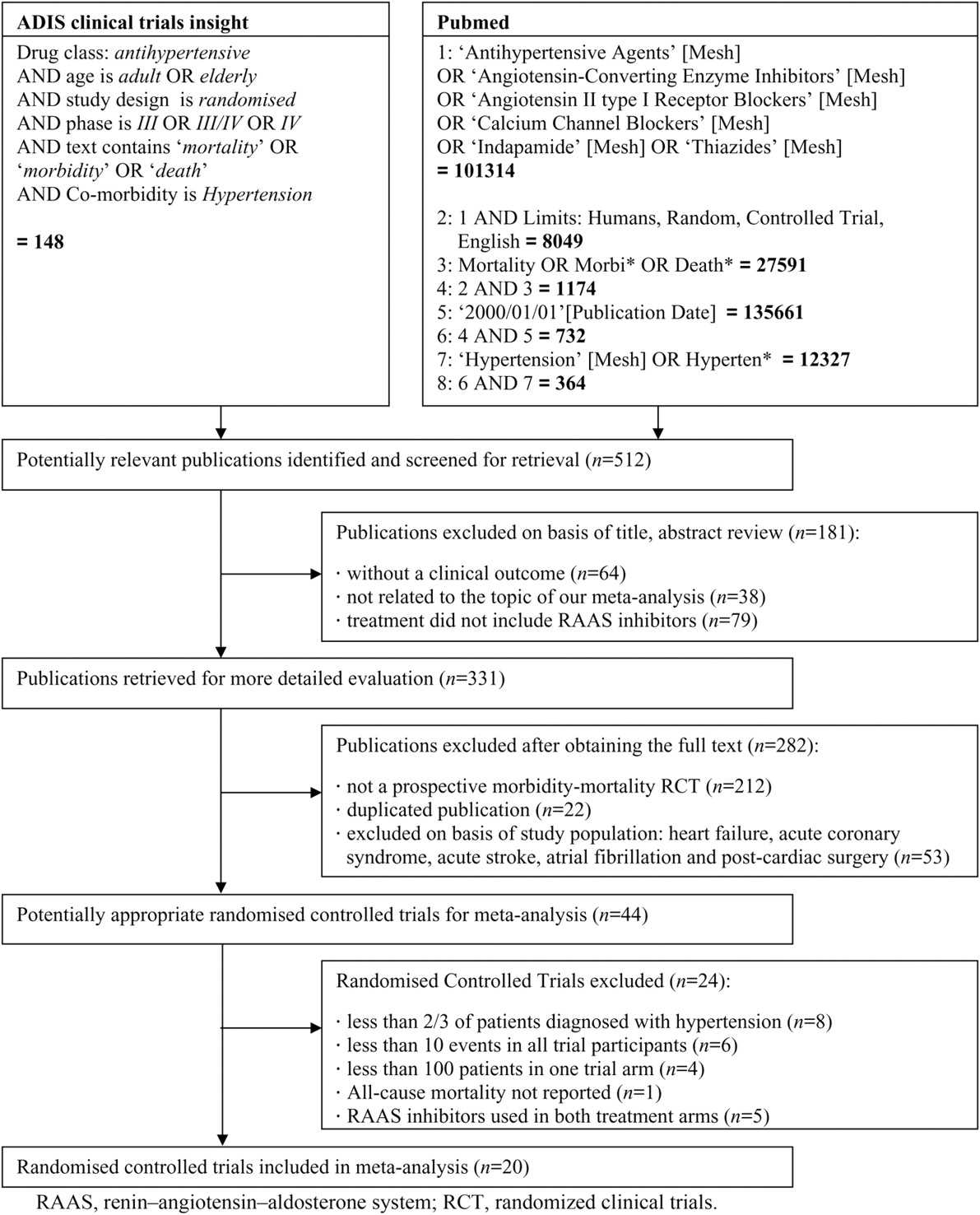

队列研究包括158998例,其中71401例应用RAAS系统抑制剂,87597例属于对照治疗。RAAS系统抑制剂和对照组的全死因死亡率分别为20.9和23.3/1000病人•年。
 eurheartj.ehs075.full.pdf
eurheartj.ehs075.full.pdfA: No. Although randomized, controlled trials have shown convincingly that angiotensin-converting enzyme (ACE) inhibitors reduce the rates of death, myocardial infarction, stroke, and heart failure in patients with known coronary artery disease or left ventricular dysfunction,1 and that angiotensin receptor blockers (ARBs) are “noninferior” to and better tolerated than ACE inhibitors, causing less angioedema and cough but costing more,2 dual renin-angiotensin system (RAS) blockade—an ACE inhibitor plus an ARB—has never been shown to reduce the rates of morbidity or death from any cause.
In fact, the Ongoing Telmisartan Alone and in Combination With Ramipril Global Endpoint Trial (ONTARGET)3,4 found that dual RAS blockade was no more beneficial than monotherapy with an ACE inhibitor or an ARB in preventing serious outcomes in patients with known vascular disease or diabetes with end-organ damage. Furthermore, patients on dual RAS blockade had higher rates of renal insufficiency, hyperkalemia, and hypotension.
Dual RAS blockade was first proposed in the early 1990s as a way to avoid the “escape phenomenon” (incomplete suppression of angiotensin II) with ACE inhibitor monotherapy.5 Indeed, studies in rats showed a synergistic effect on blood pressure with an ACE inhibitor combined with an ARB,6 and these results were encouraging enough for the medical community to make a remarkably quick transition to adopting dual RAS blockade in clinical practice.
The concept of dual RAS blockade was so appealing that effects on surrogate end points—lower blood pressure, less protein in the urine, and improved endothelial function—were accepted as free passes, obviating the need for evidence of an effect on hard end points such as lower rates of cardiovascular death or kidney failure. Currently, in the United States, about 1.5% of all patients on RAS blockers are currently receiving both an ACE inhibitor and an ARB.
Hypertension
The European Society of Cardiology’s 2007 clinical practice guidelines7 say that treatment with an ACE inhibitor plus an ARB is preferred for hypertensive patients with metabolic syndrome and its major components (eg, abdominal obesity, insulin resistance, frank diabetes).
Dulton et al, in a meta-analysis,8 calculated that the combination of an ACE inhibitor and an ARB lowered 24-hour blood pressure by 4/3 mm Hg more than monotherapy did. However, most of the studies were of short duration (6 to 8 weeks) and used submaximal doses or once-daily doses of a short-acting ACE inhibitor. Interestingly, studies that used a long-acting ACE inhibitor or a larger dose of a short-acting ACE inhibitor generally showed no additive effect on blood pressure when an ARB was added.
Hence, more evidence from larger randomized and appropriately designed studies is needed before we can conclude that dual RAS blockade is safe and significantly superior to monotherapy in blood pressure control.
Proteinuria
Proteinuria is a surrogate end point for cardiovascular death and is a marker as well as a cause of progressive renal insufficiency. It therefore seemed rational that modifying the degree of proteinuria would translate into robust clinical benefits. Several studies9 showed better renal outcomes, such as fewer patients needing dialysis with combination therapy than with an ACE inhibitor or ARB alone. However, this has never been proven in an adequately powered trial.
ONTARGET was a perfect opportunity to convert what seemed like reliable mechanistic information into solid outcome data.3 The trial enrolled 25,620 patients with established atherosclerotic disease or with diabetes and evidence of end-organ damage. At baseline, 13.1% had microalbuminuria and 4.0% had macroalbuminuria.3 The amount of protein in the urine increased by a significantly lesser amount in the ARB group and in the dualtherapy group than in the group taking only an ACE inhibitor, but in the dual-therapy group this apparent advantage came at the expense of hard end points: more patients reached the primary composite end point of needing dialysis, doubling of their serum creatinine level, or death.
Reducing proteinuria could be an important benefit, but it certainly does not outweigh the risk of increased rates of renal failure and death.
Atherosclerosis and acute coronary syndrome
The road to myocardial infarction begins with inflammation in the “shoulders” of atherosclerotic plaques, which subsequently rupture. Tissue ACE activity and expression of the angiotensin II type 1 receptor are significantly increased in patients with acute coronary syndrome and primarily co-localized to the shoulder regions of the plaque.10 Giving an ACE inhibitor or an ARB to patients who have unstable angina or who have had a myocardial infarction may decrease the rate of reinfarction and lessens the inflammatory process in the atherosclerotic plaque.
Large randomized clinical trials such as HOPE (Heart Outcomes Prevention Evaluation)11 and EUROPA (European Trial on Reduction of Cardiac Events With Perindopril in Stable Coronary Artery Disease)12 showed a lower rate of cardiovascular death in patients with established coronary artery disease and normal left ventricular function if they received an ACE inhibitor. In the HOPE trial, the rate of cardiovascular death was 25% lower in patients treated with ramipril (Altace) vs placebo.11 (The year after HOPE was published, the number of prescriptions for ramipril went up 400%). Interestingly, studies of ARBs for secondary prevention failed to show any lowering of the rate of cardiovascular death or myocardial infarction.13
In ONTARGET,4 although the combination of telmisartan (Micardis) and ramipril had a greater effect on blood pressure, it was not significantly better than ramipril alone in terms of the primary outcome of death from cardiovascular causes, myocardial infarction, stroke, or hospitalization for heart failure (relative risk 0.99).
Heart failure
The bulk of data on dual RAS blockade in heart failure patients comes from three large randomized trials: CHARM-Added (Candesartan in Heart Failure: Assessment of Reduction in Mortality and Morbidity),14 VALIANT (Valsartan in Acute Myocardial Infarction Trial),15 and VAL-HeFT (Valsartan Heart Failure Trial).16
CHARM-Added14 was the only trial that showed a reduction in cardiovascular deaths with dual RAS therapy (absolute risk reduction 3.6%). It also showed a lower rate of hospitalization for heart failure (absolute risk reduction 4%). However, the rate of allcause mortality was not different between the groups. Of note, more patients receiving dual RAS blockade had to stop taking the study drug because of adverse effects.
Val-HeFT16 showed, in a post hoc analysis, higher rates of morbidity (cardiac arrest, hospitalization for heart failure, or receipt of intravenous inotropic or vasodilator therapy for at least 4 hours) and death when the ARB valsartan (Diovan) was added to the combination of an ACE inhibitor plus a beta-blocker.
A recent meta-analysis17 of safety and tolerability of dual RAS blockade compared with an ACE inhibitor alone found a higher risk of discontinuation because of adverse effects such as hyperkalemia, renal dysfunction, and hypotension in patients on dual RAS blockade. The authors concluded that, given the adverse effects and the lack of consistent survival benefit, the available data do not support the routine addition of an ARB to ACE inhibitor therapy in heart failure patients.
WHAT ABOUT DIRECT RENIN INHIBITORS?
Another class of RAS blockers is available: direct renin inhibitors. Therefore, dual RAS blockade can be achieved by combining an ACE inhibitor with an ARB, an ACE inhibitor with a direct renin inhibitor, or an ARB with a direct renin inhibitor.
We have some outcome data on the combination of an ACE inhibitor plus an ARB,3,4,17 but none for the other two possible dual RAS combinations. Thus far, we know that dual RAS blockade with an ARB and an ACE inhibitor is not beneficial in patients like those in ONTARGET, and that it has questionable benefit in heart failure. However, little is known about combining a direct renin inhibitor with either an ACE inhibitor or an ARB.
Since ARBs and ACE inhibitors both increase plasma renin activity and only partially block the RAS, the argument has been put forward that the addition of a drug such as a direct renin inhibitor, which really decreases plasma renin activity, has the potential to be more beneficial than blockade with either an ACE inhibitor or an ARB. In theory, this is an attractive concept and certainly deserves scrutiny in outcome studies such as ALTITUDE (Aliskiren Trial in Type 2 Diabetes Using Cardio-Renal Endpoints).18
As defined by Temple,19 a surrogate end point of a clinical trial is a laboratory measurement or a physical sign used as a substitute for a clinically meaningful end point that measures directly how patients feel or function, or if they survive. Effects on surrogate end points often fail to predict the true clinical effects of an intervention, as the ONTARGET data demonstrated. Among several explanations for this failure is that interventions may affect the clinical outcome by unintended, unanticipated, and unrecognized mechanisms that operate independently of the disease process.20 Nonetheless, surrogate end point cosmetics remains attractive for many clinicians.
The ONTARGET findings indicate that there is no clinically important benefit in adding an ARB for patients with hypertension, proteinuria, heart failure, or coronary artery disease if they are already being treated with an ACE inhibitor. This would indicate that dual RAS blockade should be avoided in clinical practice until we are provided with better evidence.
本网站所有内容来源注明为“梅斯医学”或“MedSci原创”的文字、图片和音视频资料,版权均属于梅斯医学所有。非经授权,任何媒体、网站或个人不得转载,授权转载时须注明来源为“梅斯医学”。其它来源的文章系转载文章,或“梅斯号”自媒体发布的文章,仅系出于传递更多信息之目的,本站仅负责审核内容合规,其内容不代表本站立场,本站不负责内容的准确性和版权。如果存在侵权、或不希望被转载的媒体或个人可与我们联系,我们将立即进行删除处理。
在此留言





#ACE#
28
#荟萃分析#
34
#荟萃#
32
#ARBs#
35